The shoulder is a complex joint. That is involved in daily activities such as getting dressed or reaching into a cupboard. Because the shoulder is truly a ball and socket joint, providing it to move freely in six different motions, this makes it more susceptible to injury. In this article, we will review the anatomy of the shoulder, common injuries to the shoulder, functional assessments and training strategies to work with clients with previous shoulder injuries.
Functional Anatomy
Let’s look at two common functional tasks that everyone performs on a daily basis. The first is getting dressed. The movement of putting a shirt on, biomechanically, requires the shoulder to undergo initial horizontal adduction, elbow flexion, then shoulder abduction and external rotation. Anatomically, the posterior deltoid contracts during horizontal abduction, supraspinatus and medial deltoid abduct the shoulder, while teres minor and infraspinatus externally rotates the shoulder.
a. Getting dressed


Figure 1. Getting dressed Figure 2. Medial deltoid and supraspinatus
b. Reaching into cupboard
The process of reaching into the cupboard biomechanically requires shoulder flexion as seen in the figure below. Here during shoulder flexion, the humerus glides inferiorly(down) on the glenoid cavity. Anatomically, the anterior deltoid and coracobrachialis flex the shoulder.

Figure 3. Reaching into a cupboard

Figure 4. Anterior

Figure 5. Coracobrachialis
Basic anatomy
Let’s look at the shoulder anatomically There are four major joints within the shoulder complex, which include the glenohumeral joint, acromioclavicular joint, sternoclavicular joint and scapulothoracic joint.

Figure 6. Joints within the shoulder complex
Muscles
The four primary muscles that make up the rotator cuff include: supraspinatus, infraspinatus, teres minor and subscapularis. These four muscles provided stability and are involved in multiple daily activities, such as reaching, lifting, getting dressed and throwing a ball.
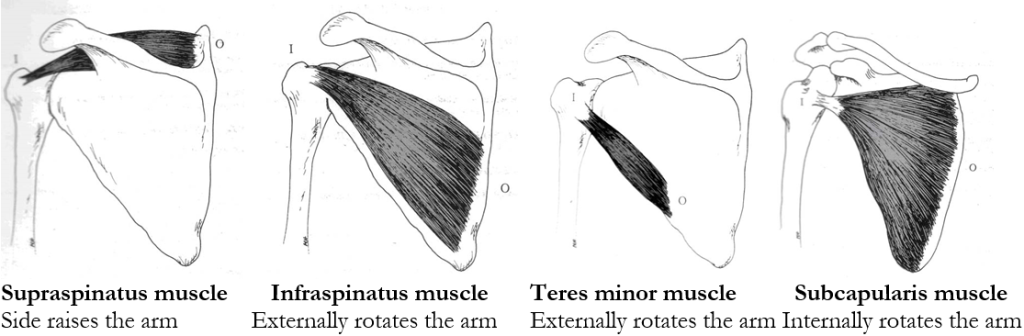
Figure 7. Rotator cuff muscles
Biomechanics
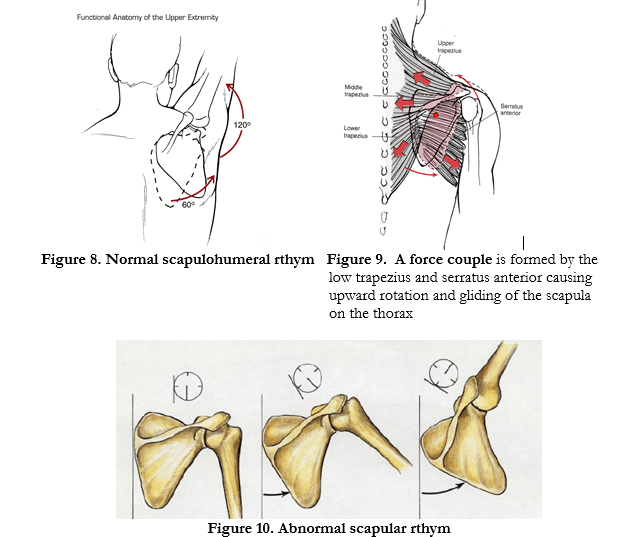
1. During shoulder flexion and abduction(side raising, there is 120 degrees of movement that occurs at the glenohumeral joint and 60 degrees at the scapulothoracic joint. This is called the scapulohumeral rhythm, (SHR) as seen in figure 8. SHR is defined as the movement relationship between the humerus and the scapula during arm raising movements.
2. As seen in figure 8, the humerus slides down in the glenoid cavity as the scapula rotates.
3. A force couple is formed during abduction(side raising) of the shoulder. The importance of this force couple(figure 9), is that when these low trapezius and searattus anterior are working synergistically, they biomechanically together cause upward rotation of the scapula on the thorax. This upward rotation of the scapula on the thorax is required to raise them arm to the side. Individuals suffering from impingement syndrome and rotator cuff repair have an altered rthym as seen in the figure below.
Common injuries and causes
There are different types of injuries the shoulder can sustain. The most common of the shoulder are impingement syndrome, rotator cuff repair and sprain,. In this next section, we will review each condition providing a deeper understanding of each.
a. Impingement syndrome
Mechanism of injury/pathophysiology: Shoulder impingement may be either primary or secondary, diagnosed by physicians. There are two types of shoulder impingement, which is
described below.
1. Primary(Mechanical) impingement: Is caused by a mechanical dysfunction such as bursa, acromioclavicular joint, acromion, humerus or rotator cuff/supraspinatus tendon beneath the coracromial arch. This is a mechanical problem that may result from sub acromial crowding.
2. Secondary(Structural) impingement: Is caused by a relative decrease in subacromial space caused by instability of the glenohumeral joint, tight posterior capsule and weakness of
scapulothoracic musculature.
• Decrease in subacromial space comprises the supraspinatus tendon, predisposing it to micro tears leading to degeneration and ultimately tearing.
• Tightness of the posterior capsule causes the humerus to migrate into theacromioclavicular joint.
• Weakness of scapulothoracic muscles leads to abnormal positioning of the scapula.
b. Rotator cuff repair
Mechanism of injury/pathophysiology: Commonly occurs as a result of a traumatic accident or fall and is graded from one to three in severity. They are classified as acute, chronic, degenerative, partial or full-thickness tears.
How dysfunctions develop:
• Impingement between the humeral head and coracromial arch occurs from repetitive loads.
• With aging(degenerative), the farthest portion of the supraspinatus tendon is particularly vulnerable to impingement or stress from overuse. Osteophytes(Calcification deposits) develop resulting in decreased sub acromial space leading to continuous micro trauma and eventual gradual tears.
• In Athletes, weakness of the rotator cuff(supraspinatus, infraspinatus particularly) results in humeral head repositioning superiorly(up) impinging the rotator cuff(RTC). This impingement leads to degenerative changes and gradual or sudden tears result.
Medical treatment: Indications for surgery, include failure to make progress after 4 to 6 months of conservative care, or an acute full-thickness tear in an active individual younger than 50 years of age.
c. Shoulder bursitis
Mechanism of injury: Bursitis occurs as a result of overuse with repeated motions to the shoulder or overhead which stresses, irritating the sub deltoid bursa and lateral shoulder musculature.
Medical treatment: Physical therapy(modalities are used such as electric stimulation to relax musculature and connective tissue as well as ROM and stretching exercises).

Figure 11. Shoulder bursitis
Common assessments
There are a few shoulder assessments that can prove to be effective.
a. Wall Push up test
With men shirt off, women wearing a sports bra, have the client place arms shoulder width on wall with feet equal distance. Instruct them to lean forward(nose towards wall) and push back to starting position. *Look for shaking or juttering of shoulder(could indicate either weakness or potential instability)
->Winging of scapula indicates weakness of serratus anterior as seen in the figure below.
Figure 12. Wall push up test
b. Reach behind back test

Figure 13. Reaching behind their back
• Instruct the client to reach behind their back and raise their hand as far as they up towards their spine.
• Mark this(the spinal segment)-serves as an objective improvement for measuring and improving internal rotation of shoulder.
• Then repeat on the opposite arm.
Training strategies and programming for shoulder injuries
a. Impingement syndrome
Recommendations for training/specific exercises with rationale:
• Continuation of posterior capsule stretching
• Strengthening serratus anterior and low trapezius together
• Scapular retraction exercises such as mid row with cable machine and low trapezius strengthening will decrease the load to front of the shoulder.
• External rotation strengthening: ideal is side lying which is more isolative for
teres minor and infraspinatus recruitment(decreases the load to the anterior shoulder).
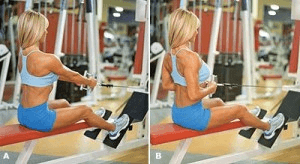
Figure 14. Seated mid row exercise

Figure 15. Low trapezius
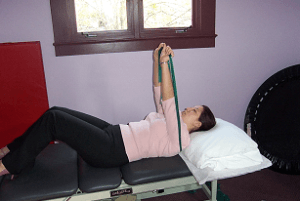
Figure 16. Serratus anterior srengthening theratubing
Exercises AVOIDED with impingement syndrome:
• Behind the neck press exercise-exercise requires the shoulder to start in a lateral and abducted position. This pulls the shoulder into a retracted position, while externally
rotated and biomechanically “impinges” the rotator cuff.
• Shoulder press creates direct axial loading to the acromioclavicular joint, supraspinatus and the sub deltoid bursa.
• Upright row-during this exercises the arm is maintained in an internally rotated position throughout the entire range of motion
b. Rotator cuff repair
Recommendations for rotator cuff training: Extremely important to consult with Orthopedic surgeon/supervising MD as well as client’s physical therapist to determine at what stage the person is. Upper body exercises that are safe based on biomechanics include:
• Low trap pull downs with cable standing or tubing
• Seated mid row, one arm DB row, seated reverse flyes(posterior deltoid)
• External rotation with cable/tubing, seated reverse flyes, seated dumbbell side raises(once medically cleared and at least 4 months tissue healing)
• Core strengthening exercises that are safe include; standing trunk rotation with cable/tubing, diagonal with cable tandem in place lunge, planks, planks with ball, trunk
rotation with forward lunge.
Exercises that are contraindicated include with rationale:
• Seated DB shoulder press(creates excessive load to the medial deltoid).
• Lat pull downs behind the head(at end or range places greatest stress on all glenohumeral ligaments as well as on the labrum).
• Barbell squats(places compressive and loading forces on the surgical graft).
• Upright row(at end of range-shoulder is maximally internally rotated which places stress on all glenohumeral ligaments, labrum and connective tissue).
• Supine dumbbell pullovers(places greatest stress on the anterior capsule and joint).
c. Shoulder Bursitis
Recommendations for training
• Continuation of stretching pectoral and upper trapezius muscles.
• Strengthening the posterior upper extremity is key. Scapular retraction exercises such as mid row with cable machine, bent over mid row, and low trapezius strengthening all decrease the load to front of the shoulder.
• External rotation strengthening: ideal is side lying which is more isolative for teres minor and infraspinatus recruitment(decreases the load to the anterior shoulder).
• Avoidance initially of shoulder press and side raises. It is important to reintegrate
these exercises slowly.
Summary
The shoulder is a complex unit that is comprised of a multitude of ligaments, tendons, connective tissue, muscles that synergistically initiate and correct movement, and stabilize when an unstable environment. Understanding the anatomy, biomechanics and weak links of the shoulder, common injuries and evidenced based training strategies, should provide you with the insight to better understand and work with clients with these kind of injuries more confidently.
Chris is the CEO of Pinnacle Training & Consulting Systems(PTCS). A continuing education company, that provides educational material in the forms of home study courses, live seminars, DVDs, webinars, articles and min books teaching in-depth, the foundation science, functional assessments and practical application behind Human Movement, that is evidenced based. Chris is both a dynamic physical therapist with 14 years experience, and a personal trainer with 17 years experience, with advanced training, has created over 10 courses, is an experienced international fitness presenter, writes for various websites and international publications, consults and teaches seminars on human movement. For more information, please visit www.pinnacle-tcs.com
REFERENCES
Cofield, R, et al. 2001, ‘Surgical Repair of Chronic Rotator Cuff Tears: A Prospective Long- Term Study,’ Journal of Bone & Joint Surgery, vol. 83-a, no. 1, pp. 23-28.
Mall, N., et al, 2010, ‘Symptomatic Progression of Asymptomatic Rotator Cuff Tears A Prospective Study of Clinical and Sonographic Variables,’ Journal of Bone and Joint Surgery,
no. 17, vol. 92, issue 16, pp. 2623-2633.
Moosmayer, S., et al., 2009, Prevalence and characteristics of asymptomatic tears of the rotator cuff: an ultrasonographic and clinical study,’ Journal of Bone and Joint Surgery,
vol. 91-B no. 2, pp. 196-200.
Nho et al., 2008, ‘Rotator cuff degeneration, etiology and pathogenesis,’ American Journal of Sports Medicine, vol. 36, number 5, pp. 987-993.
Rogers, B, et al., 2012, ‘The management of rotator cuff tears in the elderly,’ The Journal of Perioperative Practice, vol. 12, issue 1, pp. 30-32.
Sein, M., et al., 2010, ‘Shoulder pain in elite swimmers: primarily due to swim-volume- induced supraspinatus tendinopathy,’ British Journal of Sports Medicine, vol. 44, pp.105-113
Smith, M., et al., 2009, ‘Upper and lower trapezius muscle activity in subjects with sub acromial impingement symptoms: Is there imbalance and can taping change,’ Physical Therapy in Sport, pp. 1-6.
Walz, D, et al., 2007, MR imaging of delamination tears of the rotator cuff tendons, Skeletal Radiology, vol. 36, pp. 411-416.
Yamamoto, A., et al., 2010, ‘Prevalence and risk factors of a rotator cuff tear in the general population,’ Journal of Shoulder and Elbow Surgery, vol.19, issue 1, pp. 116-120.
- 30shares
- 2Facebook
- 1Twitter
- 22Pinterest
- 3LinkedIn

Chris Gellert
Latest posts by Chris Gellert
- Training the Impingement Client - August 16, 2016
- Working with the older client Part 1 - May 25, 2016
- The Cervical Spine – Understanding The Science Behind Both Movement And Dysfunction - December 10, 2014