According to the 2012 Census, people over the age of 65 make up almost 14% of the US population. That means there are over 43 million seniors (adults 65 or older) today, with the numbers continuing to grow, reaching 70 million by 2030. This aging population creates a unique opportunity for the fitness professional to work with. In this article, we will review the effects of aging on the musculoskeletal system, learn simple functional assessments and understand benefits of strength strengthening. In part 2, strength training guidelines and programming for common aging conditions will be discussed.
Effects of Aging on the Musculoskeletal System
The aging process involves changes to various structures and numerous systems within the body. Research has shown that skeletal muscles change with age, specifically type II, where there is a decreased in these fibers, that atrophy over time, and a decrease in size (Brunner et al. 2007).
Research has consistently shown that muscle strength decreases with age(Lindle RS, Metter E. 1997). Physiologically it has been studied that maximal strength capacity reaches a peak sometime around the second or third decade of life, and by the fifth decade, begins a gradual decline(Peterson et al. 2010). The strength of people in their 80s is about 40% less than that of people in their 20s(Chiung-Ju Liu, 2011). The decline in muscle strength is associated with an increased risk of falls and physical disability in older adults.
Functional assessments of older client
Balance tests
Assessing an older client’s balance needs to be objective and not guesswork. There are many tests available, but few are objective, measurable, and supported with research as the timed up and go test and sit to stand the test.
1)Timed Up and Go Test
Use a standard armchair. Place the line ten feet from the chair. The score is the time taken in seconds to complete the task. The subject is encouraged to wear regular footwear and to use any customary walking aid. No physical assistance is given.

Figure 1. TUG test
Give the following instructions:
- Rise from the chair
- Walk to the line on the floor (10 feet)
- Turn, return to the chair
- Sit down again
Scoring: Persons who take 10 seconds or less to complete this sequence of maneuvers are at low risk of falling. Persons who take >20 seconds to complete this sequence are at high risk of falling(Bohannon, RW., 2006).
2) Sit to stand test
Have the client sit with their back against the back of the chair. Ask the client to stand from the seated positing, counting each stand aloud so that the client remains oriented. Stop the test when the patient achieves the standing position on the 5th repetition. Stop the test when the patient achieves the standing position on the 5th repetition.

Figure 2. Sit to stand test Scoring-Age Norms:

Scoring-Age Norms:
3) Functional squat
The squat is a classic fundamental primal movement someone typically performs on a daily basis. Whether it is to perform to pick something up or move something. The squat is a movement that requires proper ankle and hip mobility while stability is required at the knee and lumbar spine. Understanding the functional anatomy and muscle recruitment is fundamental when prescribing this exercise with any client.

Figure 3. Squat picture
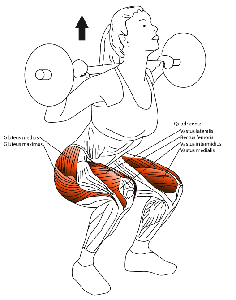
Figure 4. Squat analysis
Movement Analysis:
As the body descends, the hip flexors concentrically contract with slight lumbar flexion, while the knees undergo flexion, glute maximus and hamstrings eccentrically contract. At the ankle, dorsiflexion occurs, where the anterior tibialis(concentrically contracts) while the gastrocnemius eccentrically contracts.
Returning to an upright position(vertical), the opposite occurs. The hip flexors eccentrically contract, there is a slight lumbar extension while the knee transitions from flexion to extension. Hip extension occurs via the glute maximus while the hamstrings concentrically contract.
Ankle plantar flexion occurs with the concentric contraction of the gastrocnemius while there is an eccentric contraction of anterior tibialis.
Benefits of Strength Training for improving function in older adults
Muscles behind the movement
There are numerous benefits of strength training for older adults. However, it is important to understand the muscles behind the everyday movement. Large muscle groups, including shoulders, arms, trunk, hips and legs, are important to perform activities of daily living(ADLs) and are susceptible to the aging process, training should target these muscle groups. The latissimus dorsi muscle (assists with sit to stand). Glute maximus is a primary hip extensor muscle involved in walking and climbing stairs. The hamstring muscles are important in flexing the knee and extending the hip, which is involved in everyday activities such as walking, sit to stand, and negotiating stairs. Glute medius and minimus muscles are lateral stabilizers that are important for getting in and out of bed or car or stepping into a bathtub.

Figure 5. Glute maximus muscle

Figure 6. Glute medius muscle
Research: Benefits of Strength Training and Balance
Strength training physiologically improves the strength of bones and connective tissue, the size of fast and slow-twitch fibers, reduces blood pressure, improves blood flow with many more benefits. Research has shown specifically that strength training improves gait mechanics(Persch et al. 2009), reduces the risk for falls in the elderly (Karlson, MK et al. 2013, Trombetti, An et al. 2011, Sherrington et al. 2008 & Zhen-Bo, Cao, et al 2006).
Balance defined is defined as the ability to maintain an upright posture during both static and dynamic tasks(Benjuya, Melzer, & Kaplanski, 2004). Maintaining balance involves a complex interaction among the sensory, vestibular and visual systems.
Aging dampens reaction time and muscle strength impairing, in some people, the ability to control a fall. In older adults, possessing lateral stability is a key contributor to maintaining balance control. Lateral stability is controlled by both the glute medius and glute minimus muscles (Orr, R., et al. 2008).
It has been shown there are several contributing factors that contribute to a person with falling. One major factor is leg weakness, particularly in hamstrings and glute maximus. Which has been commonly reported as an important fall-risk factor? Individuals exhibiting this sign have 4.9 times the risk of falling than people with normal strength (Bird, L. et al., 2009, & Rubenstein, 2006).
Studies by (Nolan, M et al. 2010 and Ozcan et al. 2005 and Moreleand, JD 2004) identify that ankle mobility, specifically the lack of dorsiflexion is another contributing factor for increased falls in seniors.
Finally, several studies found that decreased plantar flexion strength is a contributing factor. (Menz et al. 2005) examined 171 men and women with a mean age 80.1, had their foot posture, the range of motion, strength, and vision, sensation, strength, reaction time, and balance examined over a 12 month period. Results: seventy-one participants (41%) reported falling during the follow-up period. Those who fell exhibited decreased ankle flexibility, decreased plantar tactile sensitivity, and decreased plantar flexor strength.
Additional factors including impaired proprioception (joint position sense), decreased flexibility and fear of falling (Visual Analogue Scale) as risk factors for falls per the research.
Summary
Aging is inevitable. Falls can be prevented. Arming yourself with more knowledge about the body will enable you to help your clients’ age gracefully reaching optimal health. A multi-component exercise intervention program that consists of strength, endurance and balance training appears to be the best strategy for improving gait, balance, and strength, as well as reducing the rate of falls in elderly individuals(Cadore, E., 2013).
REFERENCES
American Geriatrics Society and British Geriatrics Society. 2011. ‘Summary of the Updated American Geriatrics Society British Geriatrics Society Clinical Practice Guidelines for Preventions of Falls in Older Persons.’ Journal of American Geriatric Society, vol. 59., issue 1., pp.148-157.
Benjuya, Melzer, & Kaplanski, 2004, ‘Aging-induced shifts from a reliance on sensory input to muscle co-contraction during balanced standing,’ ‘The Journals of erontology,
Series A, Biological Sciences and Medical Sciences, vol. 59, issue 2, M166.
Bird, L. et al., 2009, ‘Effects of Resistance and Flexibility Exercise Interventions on Balance and Related Measures in Older Adults,’ Journal of Aging and Physical Activity, vol. 17, pp. 444-454.
Bohannon, RW., 2006, Reference values for the timed up and go test: a descriptive meta-analysis. Journal of Geriatric Physical Therapy, vol. 29, issue 2, pp.64-68.
Brunner, F., et al. 2007, ‘Effect of Aging on Skeletal Muscles,’ Journal of Aging and Physical Activity, vol. 15., pp. 336-348.
Buatois, S., et al. 2010, A simple clinical scale to stratify risk of recurrent falls in community-dwelling adults aged 65 years and older. Journal of Physical Therapy 90, vol. 4, pp. 550-556.
Cadore, E., 2013, ‘Effects of Different Exercise Interventions on Risk of Falls, Gait Ability, and Balance in Physically Frail Older Adults: A Systematic Review,’ Rejuvenation Research, Vol. 16, Number 2, pp. 105-115.
Chiung-Ju Liu, 2011, ‘Can progressive resistance strength training reduce physical disability in older adults? A meta-analysis study,’ Disability and Rehabilitation, vol. 33, issue 2., pp. 87–8.9
Karlson, MK et al. 2013, ‘Prevention of falls in the elderly: A Review,’ Osteoporosis International vol. 24. pp. 747-762.
Menz, et al. 2005, ‘Foot and Ankle Risk Factors for Falls in Older People: A Prospective Study,’ Journal of Gerontology: Biological Science, vol. 61, issue 8, pp. 866-870.
Nolan, M. et al. 2010, The Aging Male, ‘Age-related changes in musculoskeletal function, balance and mobility measures in men aged 30–80 years,’ The Aging Male, vol. 13, issue 3, pp. 194-201.
Orr, R., et al. 2008, Efficacy of Progressive Resistance Training on Balance Performance in Older Adults: A Systematic Review of Randomized Controlled Trial,’ Sports Medicine, vol. 38, issue 4, pp. 317-343.
Ozcan, A, et al. 2005, ‘The relationship between risk factors for falling and the quality of life in older adults,’ BMC series, vol. 5, issue 90.
Persch, L., et al. 2009, ‘Strength training improves fall-related gait kinematics in the elderly: A randomized controlled trial,’ Clinical Biomechanics, vol. 24, pp. 819–825.
Peterson, 2010, ‘Resistance Exercise for Muscular Strength in Older Adults: A Meta-Analysis,’ Ageing Research, vol. 9, issue 3., pp. 226-237.
Rubenstein, 2006, Falls in older people: Epidemiology, risk factors and strategies for prevention, Age and Ageing, vol. 35, supplement 2, pp. 37–41.
Sherrington, C., et al. 2008, ‘Effective Exercise for the Prevention of Falls: A Systematic Review and Meta-Analysis,’ Journal of the American Geriatrics Society, vol. 56, Issue 12, pp. 2234-2243.
Trombetti, A., 2011, ‘Effect of Music-Based Multitask Training on Gait, Balance, and Fall Risk in Elderly People A Randomized Controlled Trial,’ Archive Internal Medicine, vol. 6, pp. 525-533.
Zhen-Bo, Cao, et al 2006, ‘The Effect of a 12-week Combined Exercise Intervention Program on Physical Performance and Gait Kinematics in Community-Dwelling Elderly Women,’ Journal of Physiology Anthropology, pp. 325-330.
Was this Article Helpful?
If this article was helpful to you, please consider linking this article to your own blog or sharing this through the social buttons below. You will also find other great articles at “Expert Advice“.
- 5shares
- 5Facebook
- 0Twitter
- 0Pinterest
- 0LinkedIn

Chris Gellert
Latest posts by Chris Gellert
- Training the Impingement Client - August 16, 2016
- Working with the older client Part 1 - May 25, 2016
- The Cervical Spine – Understanding The Science Behind Both Movement And Dysfunction - December 10, 2014